
Scoliosis Treatment and Surgery
Scoliosis is a spinal disorder characterized by the curvature of the spine to the side on the vertical axis, which should normally be straight.
.avif)


Publication Date:
15/4/2026 11:35 AM

What Is Scoliosis?
Scoliosis is a spinal disorder characterized by the curvature of the spine to the side on the vertical axis, which should normally be straight. It is not only a curvature to the sides, but also a three-dimensional deformity in which the vertebrae rotate around their axis. This rotation can create pronounced asymmetry in the waist or back.
It is usually noticed in childhood and adolescence, in some cases it may not give symptoms. Adolescent idiopathic scoliosis, the most common type, occurs during adolescence and is more common in girls compared to boys. Early diagnosis is of great importance for treatment success.
What is the Cobb Angle?The severity of the curvature of the spine is determined by measuring the “Cobb angle” on the x-ray. Curvature below 10° is not considered scoliosis. It is classified as mild 10—25°, moderate 25—40°, and severe curvature above 40°. The decision to operate is usually raised in curvatures of 45—50° and above.
What Are the Symptoms of Scoliosis?
Curvature in the spine is visible to the eye in some cases or can create mild discomfort.
Symptoms to watch out for:
- Unequality at shoulder or hip levels
- Hump on the back or waist
- Unilateral back or lower back pain
- The fact that clothes do not hold properly on the body
- When leaning forward, the ribs or back muscles of one side protrude more
- Visible difference in leg lengths
Symptoms can vary significantly from person to person. While there may be no complaints with mild curvatures, chronic pain and shortness of breath can occur in advanced cases.
How is the diagnosis made?
The diagnosis of scoliosis is made by examination by a specialist physician and, if necessary, by X-ray. In the examination, the “Adam's forward bend test” is performed, in which asymmetry is observed in the rib or lumbar region.
Among the imaging methods, the full spine x-ray, which is taken standing, is the main diagnostic tool. If necessary, the spinal cord and nerve roots are also evaluated with MRI imaging. Cobb angle calculation plays a decisive role in treatment decision.
Treatment Options
The method of treatment is determined individually, based on the degree of curvature and the age of the patient.
Treatment Methods:
- Slight curvature (10°—25°): Regular follow-up and observation process. An X-ray check is sufficient every 6—12 months.
- Moderate curvature (25°—45°): The use of orthoses (corsets) to maintain the shape of the spine. The corset does not return the curvature; it slows down its progression during the growth period.
- Severe curvature (45° and above): Surgical intervention to stop the progression of curvature and restore the balance of the spine.
How is Scoliosis Surgery Done?
The main goal of scoliosis surgery is to correct the curvature as much as possible, make the correction permanent and maintain the stability of the spine.
Surgical Techniques:
- Posterior Spinal Fusion (PSF): It is the most commonly applied method. With an incision made by the back, titanium screws and rods (rods) are inserted into the curved vertebral segments. A bone graft is placed between the vertebrae, ensuring fusion over time.
- Vertebral Body Tethering (VBT) — Drawstring Scoliosis Surgery: It is a new generation technique that corrects curvature without joining bones, practiced in adolescents whose growth continues. Due to its mobility preservation, it can be preferred in suitable patients.
- Anterior Approach: In some special cases it is the type of surgery performed by reaching the spine by the abdominal or thoracic cavity.
In all scoliosis surgeries, the nerves and spinal cord are monitored instantaneously by the neuromonitoring method throughout the operation.
Recovery Process After Surgery
Although the healing process differs from patient to patient, a general framework is as follows:
- First 24—48 hours: Pain control and close monitoring in the intensive care or special care unit. The first sitting and short walking trials begin, accompanied by a physiotherapist.
- Days 2—7: Service tracking. With support, the walking distance is gradually increased. Most patients are discharged within 4—7 days.
- 2—6 weeks: Short walks at home are recommended. Prolonged sitting and driving should be avoided.
- 6—12 weeks: Desk work or return to school is possible during this period for most patients. Physiotherapy exercises begin.
- 6—12 months: Bone boiling is largely completed. Gradual return to activities such as swimming and cycling can be assessed.
- 1—2 years: Full recovery. Surgeon approval is obtained for high-intensity sports.
Recommendations for a Healthy Spine
To maintain your spine health in the long term and improve your quality of life, you can take these steps:
Practical Tips:
- Exercise regularly (swimming and pilates are especially recommended).
- In everyday life, pay attention to your posture (posture); use a chair with lumbar support for prolonged sitting.
- Distribute the weight in a balanced way, using heavy bags not on one shoulder, but with double straps.
- Maintain a healthy weight; excess weight increases the load on the lumbar vertebrae.
- Do not interrupt the checks if scoliosis has been diagnosed; an X-ray check is recommended every 6 months during the growth period and once a year in adulthood.
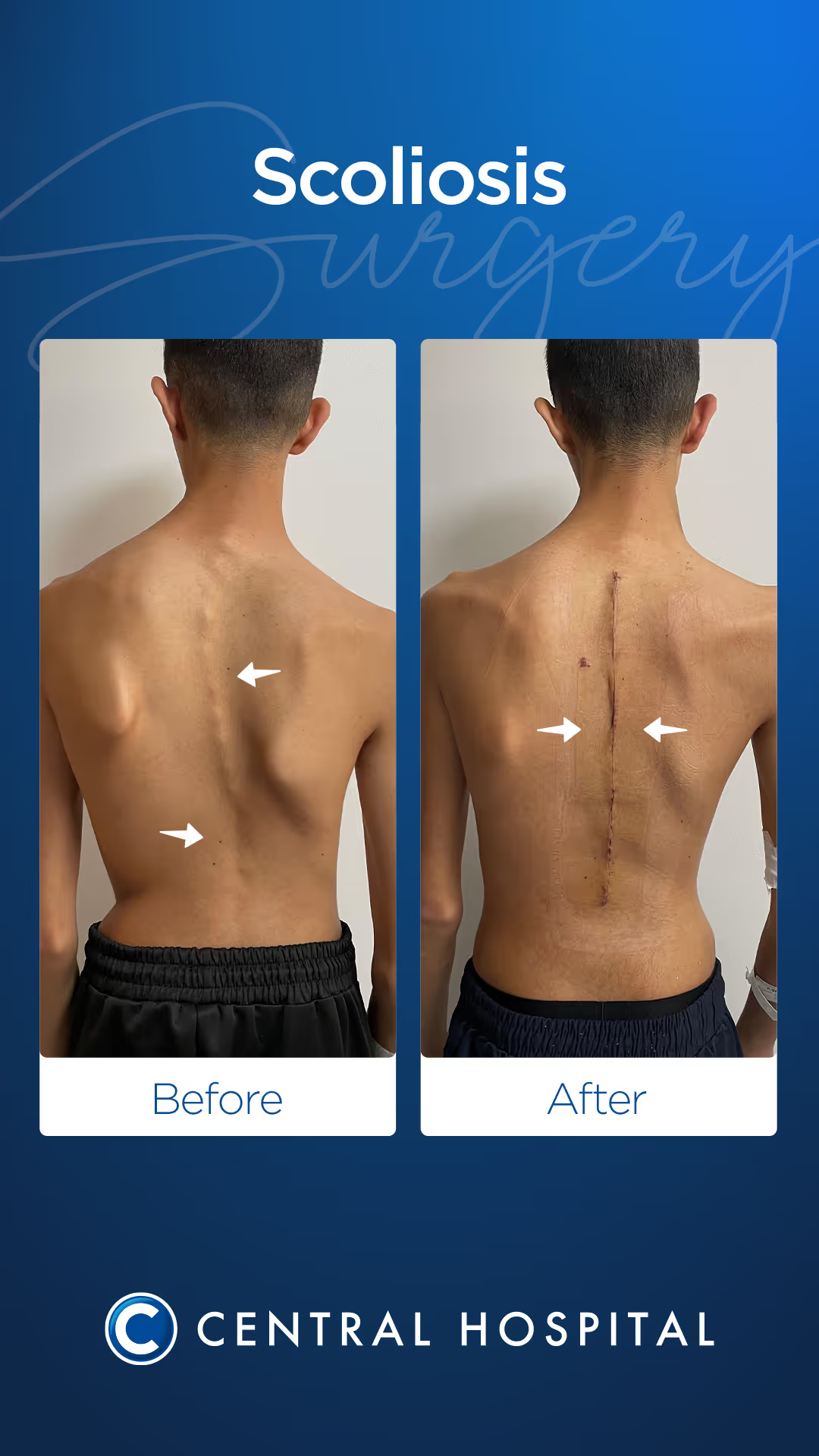
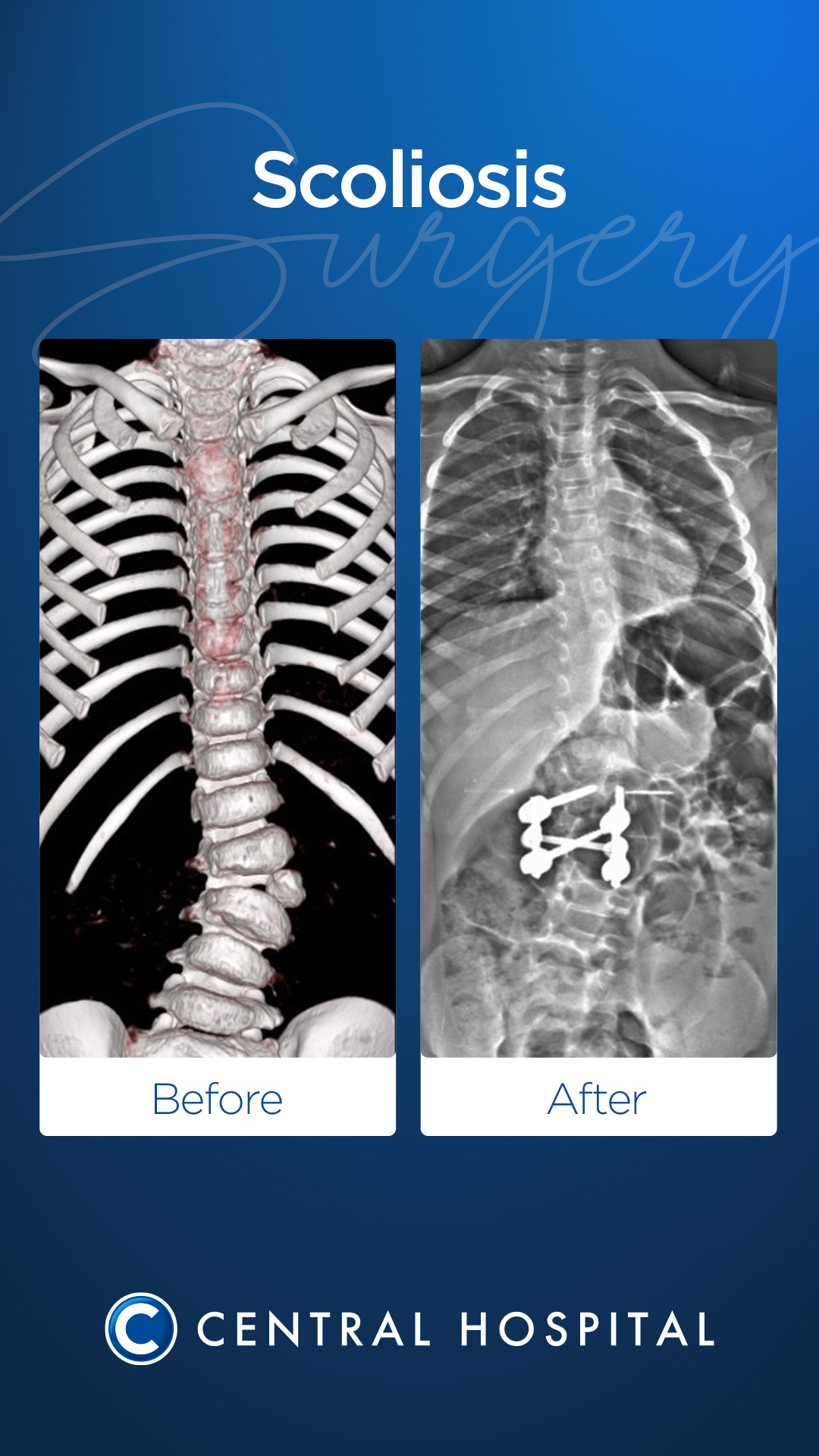
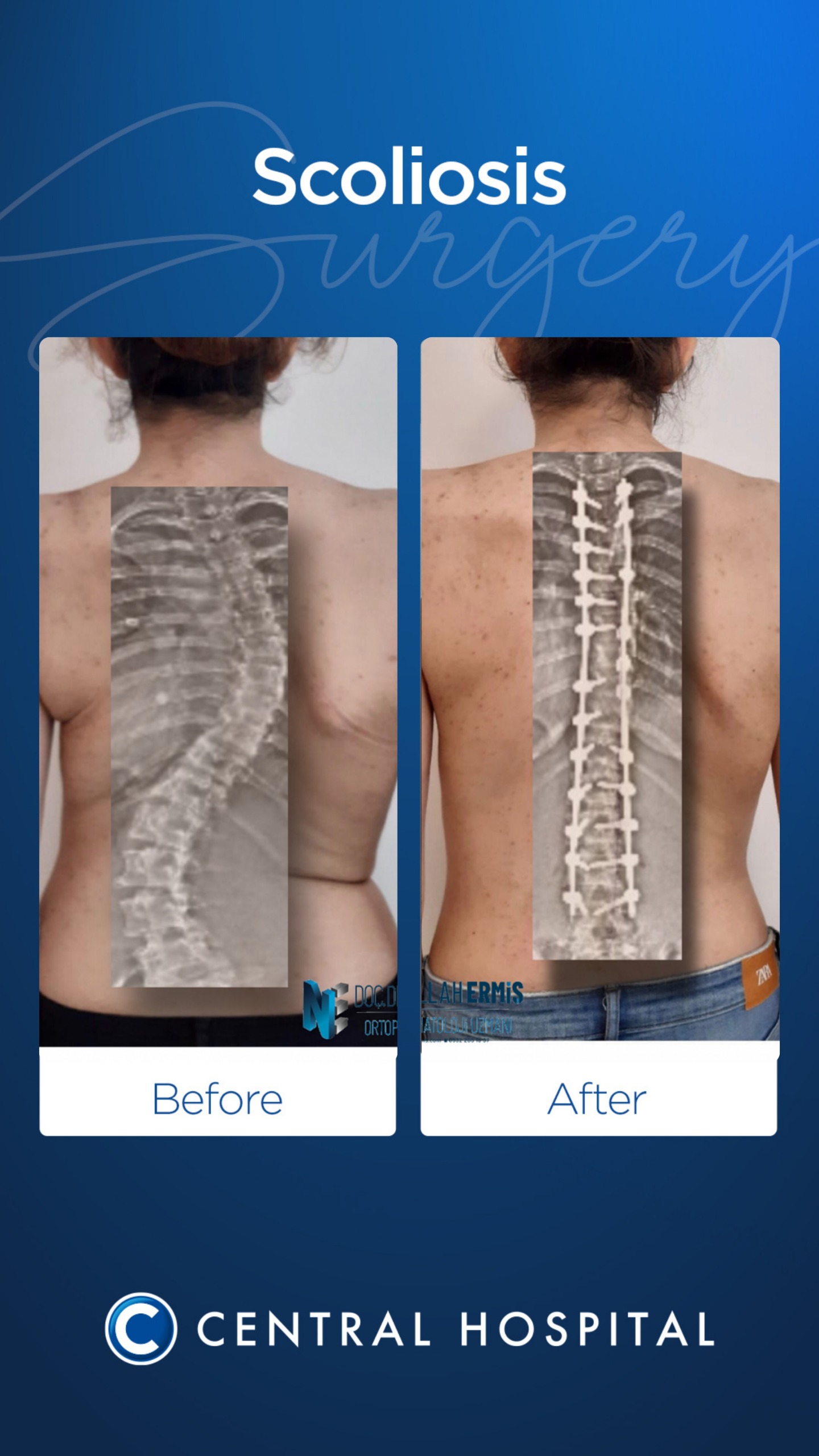
Hastalarımızın Öncesi ve Sonrası






Doctors in our unit
Easily find the doctor who best suits your needs, take a healthy step with expert support.













FAQS
We have put together frequently asked questions so that we can help you better. You can easily find the information you are looking for below
Do you still have something on your mind?
We're here! You can contact us to help you as soon as possible.